After reviewing the available literature, we are particularly concerned that certain COVID-19 vaccines may generate a pro-tumorigenic milieu (i.e., a specific environment that could lead to neoplastic transformation) that predisposes some (stable) oncologic patients and survivors to cancer progression, recurrence, and/or metastasis. This hypothesis is based on biological plausibility and fulfillment of the multi-hit hypothesis of oncogenesis (i.e., induction of lymphopenia and inflammation, downregulation of angiotensin-converting enzyme 2 (ACE2) expression, activation of oncogenic cascades, sequestration of tumor suppressor proteins, dysregulation of the RNA-G quadruplex-protein binding system, alteration of type I interferon responses, unsilencing of retrotransposable elements, etc.) together with growing evidence and safety reports filed to Vaccine Adverse Effects Report System (VAERS) suggesting that some cancer patients experienced disease exacerbation or recurrence following COVID-19 vaccination.
Experimental Approach: As persuasive theories for the underlying pathomechanisms have yet to be developed, this study investigated the effect of mRNA-1273 and BNT162b2 on the function, structure, and viability of isolated adult rat cardiomyocytes over a 72 h period.
Key Results: In the first 24 h after application, both mRNA-1273 and BNT162b2 caused neither functional disturbances nor morphological abnormalities. After 48 h, expression of the encoded spike protein was detected in ventricular cardiomyocytes for both mRNAs. At this point in time, mRNA-1273 induced arrhythmic as well as completely irregular contractions associated with irregular as well as localized calcium transients, which provide indications of significant dysfunction of the cardiac ryanodine receptor (RyR2). In contrast, BNT162b2 increased cardiomyocyte contraction via significantly increased protein kinase A (PKA) activity at the cellular level.
Conclusions and Implications: Here we demonstrated for the first time, that in isolated cardiomyocytes, both mRNA-1273 and BNT162b2 induce specific dysfunctions that correlate pathophysiologically to cardiomyopathy. Both RyR2 impairment and sustained PKA activation may significantly increase the risk of acute cardiac events.
“Experts are not entirely sure why changes in menstruation occur, but some believe the vaccine causes some of the body's tissue to become inflamed, causing changes to the lining of the uterus and hormone levels throughout the body.”
Purpose: To assess myocardial 18Fluorine-fluorodeoxyglucose (18F-FDG) uptake on PET/CT in asymptomatic SARS-CoV-2 vaccinated patients compared to nonvaccinated patients.
Results: The study included 303 nonvaccinated patients (mean age, 52.9 years ± 14.9 [SD]; 157 females) and 700 vaccinated patients (mean age, 56.8 years ± 13.7 [SD]; 344 females). Vaccinated patients had overall higher myocardial FDG uptake compared to nonvaccinated patients (median SUVmax, 4.8 [IQR: 3.0-8.5] vs median SUVmax, 3.3 [IQR: 2.5-6.2]; P < .0001). Myocardial SUVmax was higher in vaccinated patients regardless of sex (median range, 4.7-4.9 [IQR: 2.9-8.6]) or patient age (median range, 4.7-5.6 [IQR: 2.9-8.6]) compared to corresponding nonvaccinated groups (sex median range, 3.2-3.9 [IQR: 2.4-7.2]; age median range, 3.3-3.3 [IQR: 2.3-6.1]; P range, <.001-.015). Furthermore, increased myocardial FDG uptake was observed in patients imaged 1-30, 31-60, 61-120, and 121-180 days after their second vaccination (median SUVmax range, 4.6-5.1 [IQR: 2.9-8.6]) and increased ipsilateral axillary uptake was observed in patients imaged 1-30, 31-60, 61-120 days after their 2nd vaccination (median SUVmax range, 1.5-2.0 [IQR: 1.2-3.4]) compared to the nonvaccinated patients (P range, <.001-<.001).
Figure. 3: Qualitative and quantitative assessment of myocardial 18Fluroine-fluorodeoxyglucose (18F-FDG) uptake in vaccinated and nonvaccinated patients. (A) Bar plot showing the number of patients (N) who received each myocardial FDG uptake visual score (0-3) stratified by vaccination (vaccine [-], n = 303; vaccine [+], n = 700). Myocardial FDG uptake visual scores were higher in the vaccinated group compared to the unvaccinated group (Mann-Whitney U test, P < .001). (B) Boxplot showing the myocardial FDG uptake as measured by SUVmax in nonvaccinated (vaccine [-], n = 303) and vaccinated (vaccine [+], n = 700) patients. The myocardial SUVmax was higher in the vaccinated group (median, 4.8 [IQR: 3.0-8.5]) than in the unvaccinated group (median, 3.3 [IQR: 2.5-6.2]; P < .001). Horizontal bars in the boxplot represent the median SUVmax value and whiskers represent the interquartile range. The diamond in the box represents average. Mann-Whitney U test was used to compare median SUVmax values between groups.
Figure 4: Boxplots showing 18Fluroine-fluorodeoxyglucose (18F-FDG) uptake in the (A) axillary and (B) myocardium of patients stratified by the interval of time between SARS-CoV-2 vaccination and PET/CT imaging. (A) Compared to the unvaccinated group (Dose 0, median SUVmax, 1.2 [IQR: 1.0-1.4]), the axillary SUVmax was higher in patients imaged after their 1st dose (median, 1.6 [IQR: 1.3-3.2]; P <.001). Patients imaged ≤30 days (median, 2.0 [IQR: 1.6-3.4]), 31-60 days (median, 1.7 [IQR: 1.5-1.9]), and 61-120 days (median, 1.5 [IQR: 1.2-1.7]) after their 2nd dose also showed increased axillary SUVmax values compared to the unvaccinated group (P range, <.001-<.001). There was no difference observed in axillary SUVmax between unvaccinated patients and patients imaged 121-180 days (median, 1.2 [IQR: 1.0-1.5]; P = .99) or >180 days (median, 1.1 [IQR: 0.9-1.3]; P = .20) after their 2nd dose. (B) Boxplot showing myocardial SUVmax for nonvaccinated (Dose 0) and vaccinated groups. The myocardial SUVmax was higher in patients imaged after their 1st dose (median, 6.2 [IQR: 3.8-8.8]; P=.004) as well as in patients imaged 1-30 days (median, 5.1 [IQR: 3.2-8.6]), 31-60 days (median, 4.8 [IQR: 3.0-7.7]), 61-120 days (median, 4.6 [IQR: 3.2-8.5]), and 121-180 days (median, 5.1 [IQR: 2.9-8.2]) after their 2nd dose compared to the unvaccinated group (median, 3.3 [IQR: 2.5-6.2]; P range, <.001-<.001). There was no difference observed in myocardial SUVmax between unvaccinated patients and patients imaged >180 days after their 2nd dose (median, 4.5 [IQR: 2.7-9.3]; P = .15). For both boxplots, horizontal bars represent the median SUVmax value and whiskers represent the interquartile range. The diamond in the box represents average. Kruskal-Wallis test with post ad -hoc Dwass, Steel, Critchlow-Fligner multiple comparison analysis was used to compare median SUVmax values between groups.
Conclusion: Compared to nonvaccinated patients, asymptomatic patients who received their 2nd vaccination 1-180 days prior to imaging showed increased myocardial FDG uptake on PET/CT.
Experimental design: Mass spectrometry examination of biological samples was used to detect the presence of specific fragments of recombinant Spike protein in subjects who received mRNA-based vaccines.
Results: The specific PP-Spike fragment was found in 50% of the biological samples analyzed, and its presence was independent of the SARS-CoV-2 IgG antibody titer. The minimum and maximum time at which PP-Spike was detected after vaccination was 69 and 187 days, respectively.
Figure 1, D,E: (D) Time from the day of vaccination completion to the discovery of vaccine mRNA-induced Spike protein “PP”. (E) quantification of the antibody titer of the 20 vaccinated cases
According to the authors [15] and in general, the vaccine messenger RNA nanoparticle molecules should be picked up by the immune cells in the lymph nodes after injection into the muscle. Recently, other authors have isolated vaccine messenger RNA sequences from peripheral plasma after 28 days after injection [24]. The question of whether or not the vaccine RNA can be integrated into the lymphocyte or other body cells is much debated. Nonetheless, the observation of the protein produced, as presented in this manuscript, goes beyond the purely cognitive aspect and defines a method to verify not only the persistence of the vaccine RNA but the quantification of the product, that is, the protein that is supposed to induce antibody production, in order to verify the correct half-life and a possible need to update the vaccine status. Using mass spectrometry examination of biological samples, we detected the presence of specific fragments of recombinant Spike protein in about 50% of subjects who received mRNA-based vaccines. In some cases, we found the PP-Spike marker in vaccinated individuals more than 30 days after the vaccine, indicating that it is possible to detect vaccine “Spike” protein even sometime after vaccination and in any organic tissue (data in preparation). Based on the results obtained, hypotheses can be made for possible molecular mechanisms of persistence of “Spike PP.” In particular, three hypotheses are possible and are shown in Figure 3.
It is possible that the mRNA may be integrated or re-transcribed in some cells.
It is possible that pseudo-uridines at a particular sequence position, as described in the article, induce the formation of a spike protein that is always constitutively active. But it seems very remote as a hypothesis.
It is possible that the mRNA-containing nanoparticle will be picked up by bacteria normally present at the basal level in the blood. In fact, the existence of blood microbiota in clinically healthy individuals was proven during the last 50 years. Indeed, indirect evidence by radiometric analyses suggested the existence of living microbial forms in erythrocytes [25]. In addition, the observation of the PP-Spike marker in individuals vaccinated more than 30 days after the vaccine in about 50% of subjects could also be explained by the wide biodiversity of eukaryotic and prokaryotic microbiota identified in blood by next-generation sequencing technologies [25].
Figure3. Possible molecular mechanisms of persistence of “Spike PP”.
Here we investigated whether spike protein binding to ACE2 induces inflammation in endothelial cells and determined the role of ACE2 in this process. Human endothelial cells were exposed to SARS-CoV-2 spike protein, S1 subunit (rS1p) and pro-inflammatory signaling and inflammatory mediators assessed. ACE2 was modulated pharmacologically and by siRNA. Endothelial cells were also exposed to SARS-CoV-2. rSP1 increased production of IL-6, MCP-1, ICAM-1 and PAI-1, and induced NFkB activation via ACE2 in endothelial cells.rS1p increased microparticle formation, a functional marker of endothelial injury. ACE2 interacting proteins involved in inflammation and RNA biology were identified in rS1p-treated cells. Neither ACE2 expression nor ACE2 enzymatic function were affected by rSP1. Endothelial cells exposed to SARS-CoV-2 virus did not exhibit viral replication. We demonstrate that rSP1 induces endothelial inflammation via ACE2 through processes that are independent of ACE2 enzymatic activity and viral replication.
rS1p induces endothelial cell inflammation and injury. Proteomic analysis of rS1p-treated endothelial cells. (A) The figure represents 1150 hMEC protein interactome created by STRING. Each circular dot (blue, pink) represents the node (protein) and the grey lines the edges. (B) represents the heat map of differentially expressed proteins after 24 h of recombinant S1 spike protein (rS1p). Shades of blue represent the z-score intensities (scale below the heat map). Grey shade represents missing intensities. Human endothelial cells (hMEC) were stimulated with rS1p (0.66 μg/mL) for 5 h and 24 h for assessment of IL-6 (C) and MCP-1 (D) mRNA expression; IL-6 (E) and MCP-1 (F) production. Data are expressed as ± SEM; *p < 0.05 control (Ctl) (non-stimulated cells) vs. rS1p stimulated cells after student’s t-test.
Results:SARS-CoV-2 recombinant S1 protein induces endothelial inflammation and cell damage independently of viral infection.
Aim: To investigate heterologous and specific immunological effects of BNT162b2 COVID-19 vaccination in children.
Methods: A whole blood stimulation assay was used to investigate in vitro cytokine responses to heterologous stimulants (killed pathogens, Toll-like receptor ligands) and SARS-CoV-2 antigens. Samples from 29 children, aged 5-11 years, before and 28 days after a second BNT162b2 vaccination were analysed (V2 + 28). Samples from eight children were analysed six months after BNT162b2 vaccination.
Results: At V2 + 28, interferon-γ and monocyte chemoattractant protein-1 responses to S. aureus, E. coli, L. monocytogenes, BCG vaccine, H. influenzae, hepatitis B antigen, poly(I:C) and R848 stimulations were decreased compared to pre-vaccination. For most of these heterologous stimulants, IL-6, IL-15 and IL-17 responses were also decreased. There were sustained decreases in cytokine responses to viral, but not bacterial, stimulants six months after BNT162b2 vaccination. Cytokine responses to irradiated SARS-CoV-2, and spike glycoprotein subunits (S1 and S2) were increased at V2 + 28 for most cytokines and remained higher than pre-vaccination responses 6 months after BNT162b2 vaccination for irradiated SARS-CoV-2 and S1. There was no correlation between BNT162b2 vaccination-induced anti-SARS-CoV2-receptor binding domain IgG antibody titre at V2 + 28 and cytokine responses.
A growing number of leprosy cases are being reported after COVID-19 vaccination, including two cases in the United Kingdom that researchers said may have been caused by the vaccines.
The researchers examined records from the Leprosy Clinic at the Hospital for Tropical Diseases in London. They found that of the 52 people who went to the clinic in 2021, at least 49 were vaccinated.
The study definition of a leprosy adverse event associated with a COVID-19 vaccine included developing leprosy or a leprosy reaction within 12 weeks of receiving a dose and the person having no previous history of leprosy or a leprosy reaction.
Two people met the case definition. One developed borderline tuberculoid (BT) leprosy one week after a second dose. The other experienced a reaction 56 days after a dose. Both doses were Pfizer’s BNT162b2 vaccine. Pfizer did not respond to a request for comment.
“The development of BT leprosy and a Type 1 reaction in another individual shortly after a dose of BNT162b2 vaccine may be associated with vaccine mediated T cell responses,” the researchers said.
The COVID-19 vaccines can provoke a response from white blood cells, or T cells. The cells are believed to protect against COVID-19.
T-cells can theoretically trigger Mycobacterium leprae, a bacteria that causes leprosy, leading to leprosy or a leprosy reaction, the researchers said.
Other vaccines have been shown to trigger leprosy or leprosy reactions, including tuberculosis vaccines, and some people who receive repeated COVID-19 vaccinations have been shown to have weakened immune systems.
A skilled nursing facility (SNF) with an average of 152 residents administered the COVID vaccines to employees and residents on Dec 28 & 29, 2020. Between Jan 2 and Jan 20, 2021, approximately 42+ residents died. The management had to interrupt the staff’s holiday to call them back to work due to all the deaths. Here’s the kicker: In all of 2020, this facility had ZERO COVID deaths. The average in-SNF annual mortality rate at SNFs is 7.8% (see Table 3). That means that the chance of seeing 42 or more deaths in a 20-day window with 152 residents (where we’d normally see .65 deaths) is given by:
>>> poisson.sf(41, .65) 5.236053428716437e-60
In other words, this is not simply a statistical outlier. There is absolutely no way these deaths weren’t COVID vaccine related.
There was no news coverage of this and nobody has ever leaked this story to the press. Until just now.
Whilst there has been significant public health benefits associated with global use of COVID-19 spike protein vaccines, potential serious adverse events following immunization have been reported. Acute myocarditis is a rare complication of COVID19 vaccines and often it is self-limiting. We describe two cases experiencing recurrent myocarditis following mRNA COVID-19 vaccine despite a prior episode with full clinical recovery. Between September 2021-September 2022 we observed two male adolescents with recurrent myocarditis related to mRNA-based-COVID19 vaccine. During the first episode both patients presented with fever and chest pain few days after their second dose of BNT162b2 mRNA Covid-19 Vaccine (Comirnaty®). The blood exams showed increased cardiac enzymes. In addition, complete viral panel was run, showing HHV7 positivity in a single case. The left ventricular ejection fraction (LVEF) was normal at echocardiogram but cardiac magnetic resonance scanning (CMR) was consistent with myocarditis. They were treated with supportive treatment with full recovery. The 6 months follow-up demonstrated good clinical conditions with normal cardiological findings. The CMR showed persistent lesions in left ventricle ‘s wall with LGE. After some months the patients presented at emergency department with fever and chest pain and increased cardiac enzymes. No decreased LVEF was observed. The CMR showed new focal areas of edema in the first case report and stable lesions in the second one. They reached full recovery with normalization of cardiac enzymes after few days. These case reports outline the need of strict follow-up in patients with CMR consistent with myocarditis after mRNA-based-COVID19 vaccine. More efforts are necessary to depict the underlying mechanisms of myocarditis after SARS-CoV2 vaccination to understand the risk of relapsing and the long-term sequelae.
Experimental design: Mass spectrometry examination of biological samples was used to detect the presence of specific fragments of recombinant Spike protein in subjects who received mRNA-based vaccines.
Results: The specific PP-Spike fragment was found in 50%of the biological samples analyzed, and its presence was independent of the SARS-CoV-2 IgG antibody titer. The minimum and maximum time at which PP-Spike was detected after vaccination was 69 and 187 days, respectively.
Thirty-nine patients had CMR at presentation, 26 of whom had abnormal findings. These included features of myocarditis in 22 (56%), abnormal T1 values in 21 (54%), abnormal T2 values in 24 (62%), late gadolinium enhancement (LGE) in 19 (49%), and reduced LVEF in 7 (18%). The CMR-derived LVEF at initial assessment correlated with LV 4-chamber longitudinal (r=0.36, P=0.04), global longitudinal (r=0.41, P=0.02), and circumferential (r=0.38, P=0.03) absolute systolic strain at follow-up echocardiography. Follow-up CMR performed in 26 patients with initial abnormal CMR findings revealed mild residual LGE in 15 (58%; Figure B), borderline LVEF in 2 (8%), and normal findings in 11 (42%) patients.
C. Distribution of cardiac magnetic resonance late gadolinium enhancement based on the 17-segment model. LV indicates left ventricular; and RV, right ventricular.
The implications of impaired systolic and diastolic myocardial deformation and LGE in our patient subset remain unclear. Nonetheless, given that impaired myocardial deformation and LGE are indicators of subclinical myocardial dysfunction and fibrosis, there exists a potential long-term effect on exercise capacity and cardiac functional reserve during stress.
A Lancet review of 325 autopsies after Covid vaccination found that 74% of the deaths were caused by the vaccine – but the study was removed within 24 hours.
The original study abstract can be found in the Internet Archive. It reads:
Background: The rapid development and widespread deployment of COVID-19 vaccines, combined with a high number of adverse event reports, have led to concerns over possible mechanisms of injury including systemic lipid nanoparticle (LNP) and mRNA distribution, spike protein-associated tissue damage, thrombogenicity, immune system dysfunction and carcinogenicity. The aim of this systematic review is to investigate possible causal links between COVID-19 vaccine administration and death using autopsies and post-mortem analysis.
Methods: We searched for all published autopsy and necropsy reports relating to COVID-19 vaccination up until May 18th, 2023. We initially identified 678 studies and, after screening for our inclusion criteria, included 44 papers that contained 325 autopsy cases and one necropsy case. Three physicians independently reviewed all deaths and determined whether COVID-19 vaccination was the direct cause or contributed significantly to death.
Findings: The most implicated organ system in COVID-19 vaccine-associated death was the cardiovascular system (53%), followed by the hematological system (17%), the respiratory system (8%) and multiple organ systems (7%). Three or more organ systems were affected in 21 cases. The mean time from vaccination to death was 14.3 days. Most deaths occurred within a week from last vaccine administration. A total of 240 deaths (73.9%) were independently adjudicated as directly due to or significantly contributed to by COVID-19 vaccination.
Interpretation: The consistency seen among cases in this review with known COVID-19 vaccine adverse events, their mechanisms and related excess death, coupled with autopsy confirmation and physician-led death adjudication, suggests there is a high likelihood of a causal link between COVID-19 vaccines and death in most cases. Further urgent investigation is required for the purpose of clarifying our findings.
The full study does not appear to have been saved in the Internet Archive, but can be read here.
COVID-19 vaccine-related myocarditis (VRM) was confirmed in 480 cases (1.08 cases per 100 000 persons). Vaccination-related myocarditis incidence was significantly higher in men than in women (1.35 vs. 0.82 per 100 000 persons, P < 0.001) and in mRNA vaccines than in other vaccines (1.46 vs. 0.14 per 100 000 persons, P < 0.001). Vaccination-related myocarditis incidence was highest in males between the ages of 12 and 17 years (5.29 cases per 100 000 persons) and lowest in females over 70 years (0.16 cases per 100 000 persons). Severe VRM was identified in 95 cases (19.8% of total VRM, 0.22 per 100 000 vaccinated persons), 85 intensive care unit admission (17.7%), 36 fulminant myocarditis (7.5%), 21 extracorporeal membrane oxygenation therapy (4.4%), 21 deaths (4.4%), and 1 heart transplantation (0.2%). Eight out of 21 deaths were sudden cardiac death (SCD) attributable to VRM proved by an autopsy, and all cases of SCD attributable to VRM were aged under 45 years and received mRNA vaccines.
Emerging evidence suggests that the reported increase in IgG4 levels detected after repeated vaccination with the mRNA vaccines may not be a protective mechanism; rather, it constitutes an immune tolerance mechanism to the spike protein that could promote unopposed SARS-CoV2 infection and replication by suppressing natural antiviral responses. Increased IgG4 synthesis due to repeated mRNA vaccination with high antigen concentrations may also causeautoimmune diseases, and promote cancer growth and autoimmune myocarditis in susceptible individuals.
Individuals with COVID-19 vaccination had a higher risk of all forms of retinal vascular occlusion in 2 years after vaccination, with an overall hazard ratio of 2.19 (95% confidence interval 2.00–2.39). The cumulative incidence of retinal vascular occlusion was significantly higher in the vaccinated cohort compared to the unvaccinated cohort, 2 years and 12 weeks after vaccination. The risk of retinal vascular occlusion significantly increased during the first 2 weeks after vaccination and persisted for 12 weeks. Additionally, individuals with first and second dose of BNT162b2 and mRNA-1273 had significantly increased risk of retinal vascular occlusion 2 years following vaccination, while no disparity was detected between brand and dose of vaccines. This large multicenter study strengthens the findings of previous cases. Retinal vascular occlusion may not be a coincidental finding after COVID-19 vaccination.
We examined rates of SAEs between different BNT162b2 vaccine batches administered in Denmark (population 5.8 million) from 27 December 2020 to 11 January 2022. Since the observed relationship between the numbers of SAEs and BNT162b2 vaccine doses was highly heterogeneous, conventional regression statistics were not considered to be applicable. Therefore, heterogeneity in the relationship between the numbers of SAEs and doses per vaccine batch was assessed by log-transformation followed by non-hierarchical cluster analysis and general linear model (GLM) test for differences in SAE rates between batches.
Three predominant trendlines were discerned, with noticeable lower SAE rates in larger vaccine batches and additional batch-dependent heterogeneity in the distribution of SAE seriousness between the batches representing the three trendlines (Figure 1). Compared to the rates of all SAEs, serious SAEs and SAE-related deaths per 1.000 doses were much less frequent and numbers of these SAEs per 1000 doses displayed considerably greater variability between batches, with lesser separation between the three trendlines (not shown):
Figure1. Numbers of suspected adverse events (SAEs) after BNT612b2 mRNA vaccination in Denmark (27 December 2020–11 January 2022) according to the number of doses per vaccine batch. Each dot represents a single vaccine batch. Trendlines are linear regression lines. Blue: R2 = 0.78, β = 0.0898 (95% confidence interval [CI] 0.0514–0.1281), green: R2 = 0.89, β = 0.0025 (95% CI 0.0021–0.0029), yellow: R2 = 0.68, β = 0.000087 (95% CI 0.000056–0.000118). Vaccine batches representing the blue, green and yellow trendlines comprised 4.22%, 63.69% and 32.09% of all vaccine doses, respectively, with 70.78%, 27.49% and 47.15% (blue trendline), 28.84%, 71.50% and 51.99% (green trendline), and 0.38%, 1.01%, and 0.86% (yellow trendline) of all SAEs, serious SAEs, and SAE-related deaths, respectively.
“Risk assessment of retinal vascular occlusion after COVID-19 vaccination” (2023.05.02):
Abstract. …Individuals with COVID-19 vaccination had a higher risk of all forms of retinal vascular occlusion in 2 years after vaccination, with an overall hazard ratio of 2.19 (95% confidence interval 2.00–2.39). The cumulative incidence of retinal vascular occlusion was significantly higher in the vaccinated cohort compared to the unvaccinated cohort, 2 years and 12 weeks after vaccination. The risk of retinal vascular occlusion significantly increased during the first 2 weeks after vaccination and persisted for 12 weeks. Additionally, individuals with first and second dose of BNT162b2 and mRNA-1273 had significantly increased risk of retinal vascular occlusion 2 years following vaccination, while no disparity was detected between brand and dose of vaccines. This large multicenter study strengthens the findings of previous cases. Retinal vascular occlusion may not be a coincidental finding after COVID-19 vaccination.
A 14-year-old Japanese girl died unexpectedly 2 days after receiving the third dose of the BNT1262b2 mRNA COVID-19 vaccine. Autopsy findings showed congestive edema of the lungs, T-cell lymphocytic and macrophage infiltration in the lungs, pericardium, and myocardium of the left atria and left ventricle, liver, kidneys, stomach, duodenum, bladder, and diaphragm. Since there was no preceding infection, allergy, or drug toxicity exposure, the patient was diagnosed with post-vaccination pneumonia, myopericarditis, hepatitis, nephritis, gastroenteritis, cystitis, and myositis.
The researchers linked immunization records to deaths from any cause recorded in people age 12 to 29. They looked at data starting Dec. 8, 2020, when the vaccines were rolled out in Britain. The mortality data came from two independent sources: deaths registered by June 8, 2022, and hospital deaths by March 31, 2022.
The analysis found six cardiac-related deaths per 100,000 young women who received at least one dose of the vaccine in Britain. In these women, the cardiac-related death was 3.5 times more likely in the 12 weeks following vaccination than after the 12-week period. Clots that block blood flow can cause a heart attack or stroke.
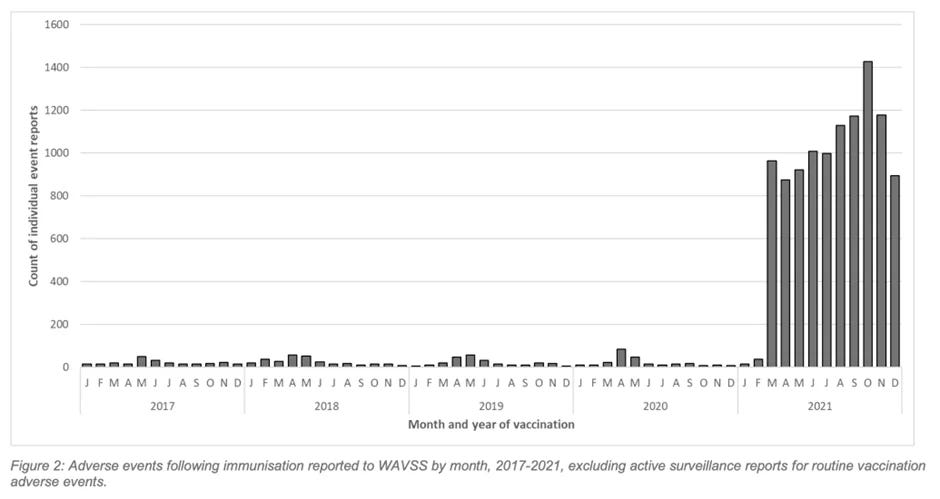
Isolated from the rest of the world, the Australian state of Western Australia (WA) managed to keep Covid out for most of 2021. During that time, almost four million doses of Covid vaccine were administered to the population. WA’s vaccine safety surveillance report for 2021 has just been released and the results are grim: an ‘exponential increase’ in adverse events, with hospitals struggling to cope.
Background: Cases of adolescents and young adults developing myocarditis after vaccination with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-targeted mRNA vaccines have been reported globally, but the underlying immunoprofiles of these individuals have not been described in detail.
Methods: From January 2021 through February 2022, we prospectively collected blood from 16 patients who were hospitalized at Massachusetts General for Children or Boston Children's Hospital for myocarditis, presenting with chest pain with elevated cardiac troponin T after SARS-CoV-2 vaccination. We performed extensive antibody profiling, including tests for SARS-CoV-2-specific humoral responses and assessment for autoantibodies or antibodies against the human-relevant virome, SARS-CoV-2-specific T-cell analysis, and cytokine and SARS-CoV-2 antigen profiling. Results were compared with those from 45 healthy, asymptomatic, age-matched vaccinated control subjects.
Results: Extensive antibody profiling and T-cell responses in the individuals who developed postvaccine myocarditis were essentially indistinguishable from those of vaccinated control subjects, despite a modest increase in cytokine production. A notable finding was that markedly elevated levels of full-length spike protein (33.9±22.4 pg/mL), unbound by antibodies, were detected in the plasma of individuals with postvaccine myocarditis, whereas no free spike was detected in asymptomatic vaccinated control subjects (unpaired t test; P<0.0001).
Conclusions: Immunoprofiling of vaccinated adolescents and young adults revealed that the mRNA vaccine-induced immune responses did not differ between individuals who developed myocarditis and individuals who did not. However, free spike antigen was detected in the blood of adolescents and young adults who developed post-mRNA vaccine myocarditis, advancing insight into its potential underlying cause.
Figure 4. This is an expanded version of Fig. 1. Your risk of death after shot #2 peaks at 4 months after the shot. If this were a safe vaccine, all the bars would be the SAME height.
Research shows that, for Europe, C19 “Vaccines” kill 3-4 times more than C19 Disease: On page 7 of 23 of the report, we have this: “...covid IFR is in the order of 0.1%.”
Vaccine Fatality Ratio (VFR) results are 0.13% (0.05%-0.21%, 95% confidence interval) in The Netherlands and 0.35% (0.15%-0.55%) in Europe, subtantially transcending covid IFR. Additionally, sewer-viral-particle experiments suggested vaccination induces covid-infections and/or reactivates latent viral reservoirs. The evidence of a causal relationship from vaccination to both infection and mortality is a very strong alarm signal to immediately stop current mass vaccination programmes.
“GAME OVER: Medicare data shows the COVID vaccines increase your risk of dying” (Steve Kirsch, 2023.02.25):
The record-level vax-death Medicare data I received is now publicly available. Now, for the very first time, you can analyze it yourself.
It shows the vaccines increase the risk of death for the elderly and that these risks appear to remain persistently elevated. It’s anyone’s guess for how long.
So now you know why the CDC never showed us the Medicare data. And now you know why the medical community and mainstream media never asked to see it and never will. They had it the whole time and kept it from public view so they wouldn’t create “vaccine hesitancy.”
If you think public health officials don’t hide the data, you should read this tweet from Chris Martenson where the Australian health authorities admit that they covered up vaccine deaths because they “didn’t want to undermine public confidence” in the vaccine. Get it?
If you think public health officials in the US want to see all the safety data even for just themselves, you should watch my video of Stanford Professor Grace Lee calling the Palo Alto Police on me when I tried to ask her if she wanted to see the safety data from the Israeli Ministry of Health.
Basically, the health authorities in the US run the other way when you try to confront them with data showing they are wrong. The proof is on that video. I tried to show the top CDC outside official world-class data collected by top scientists hand-picked by the Israeli health authorities. And her response to my offer to see the data was to call the cops.
Finally, if your doctor still tells you to take the shot, ask her to first explain to you why the slope in the Medicare data goes the wrong way before you get the shot. Have her explain to you why all these charts in this article are “normal.” And let us all know what she says in the comments.
Background: Cases of adolescents and young adults developing myocarditis after vaccination with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)–targeted mRNA vaccines have been reported globally, but the underlying immunoprofiles of these individuals have not been described in detail.
Methods: From January 2021 through February 2022, we prospectively collected blood from 16 patients who were hospitalized at Massachusetts General for Children or Boston Children’s Hospital for myocarditis, presenting with chest pain with elevated cardiac troponin T after SARS-CoV-2 vaccination. We performed extensive antibody profiling, including tests for SARS-CoV-2–specific humoral responses and assessment for autoantibodies or antibodies against the human-relevant virome, SARS-CoV-2–specific T-cell analysis, and cytokine and SARS-CoV-2 antigen profiling. Results were compared with those from 45 healthy, asymptomatic, age-matched vaccinated control subjects.
Results: Extensive antibody profiling and T-cell responses in the individuals who developed postvaccine myocarditis were essentially indistinguishable from those of vaccinated control subjects, despite a modest increase in cytokine production. A notable finding was that markedly elevated levels of full-length spike protein (33.9±22.4 pg/mL), unbound by antibodies, were detected in the plasma of individuals with postvaccine myocarditis, whereas no free spike was detected in asymptomatic vaccinated control subjects (unpaired t test; P<0.0001).
Conclusions: Immunoprofiling of vaccinated adolescents and young adults revealed that the mRNA vaccine–induced immune responses did not differ between individuals who developed myocarditis and individuals who did not. However, free spike antigen was detected in the blood of adolescents and young adults who developed post-mRNA vaccine myocarditis, advancing insight into its potential underlying cause.
Results:COVID-19 vaccines, when compared to the Influenza vaccines are associated with a significant increase in AE with all proportional reporting ratios of > 2.0: menstrual abnormality, miscarriage, fetal chromosomal abnormalities, fetal malformation, fetal cystic hygroma, fetal cardiac disorders, fetal arrhythmia, fetal cardiac arrest, fetal vascular mal-perfusion, fetal growth abnormalities, fetal abnormal surveillance, fetal placental thrombosis, low amniotic fluid, and fetal death/stillbirth (all p values were much smaller than 0.05). When normalized by time-available, doses-given, or persons-received, all COVID-19 vaccine AE far exceed the safety signal on all recognized thresholds.Conclusions:Pregnancy and menstrual abnormalities are significantly more frequent following COVID-19 vaccinations than that of Influenza vaccinations. A worldwide moratorium on the use of COVID-19 vaccines in pregnancy is advised until randomized prospective trials document safety in pregnancy and long-term follow-up in offspring.
Individuals admitted to hospital for myocarditis within 28 days of vaccination with a SARS-CoV-2 mRNA vaccine (any dose) were categorised as having myocarditis associated with vaccination; individuals admitted to hospital for myocarditis within 28 days of a positive polymerase chain reaction (PCR) test result for the SARS-CoV-2 virus were categorised as having myocarditis associated with covid-19 disease. The remaining patients who were admitted to hospital for myocarditis were categorised as conventional myocarditis. If an individual had received an mRNA vaccine and had a positive PCR test result for SARSCoV-2 infection within 28 days, the latest exposure defined the type of myocarditis. Information on mRNA vaccinations for the SARS-CoV-2 virus were obtained from national vaccination registries in each country, and information on positive PCR test results were taken from national infectious disease surveillance registries (online supplemental table S3).
In 2018-22, 7292 patients were admitted to hospital with new onset myocarditis, with 530 (7.3%) categorised as having myocarditis associated with SARS-CoV-2 mRNA vaccination, 109 (1.5%) with myocarditis associated with covid-19 disease, and 6653 (91.2%) with conventional myocarditis.
At the 90 day follow-up, 62, 9, and 988 patients had been readmitted to hospital in each group (vaccination, covid-19, and conventional myocarditis groups, respectively), corresponding to a relative risk of readmission of 0.79 (95% confidence interval 0.62 to 1.00) and 0.55 (0.30 to 1.04) for the vaccination type and covid-19 type myocarditis groups, respectively, compared with the conventional myocarditis group.
We evaluated 14 outcomes of interest following COVID-19 vaccination using the US Centers for Medicare & Medicaid Services (CMS) data covering 30,712,101 elderly persons. The CMS data from December 11, 2020 through Jan 15, 2022 included 17,411,342 COVID-19 vaccinees who received a total of 34,639,937 doses. We conducted weekly sequential testing and generated rate ratios (RR) of observed outcome rates compared to historical (or expected) rates prior to COVID-19 vaccination.
Four outcomes met the threshold for a statistical signal following BNT162b2 vaccination including pulmonary embolism (PE; RR = 1.54), acute myocardial infarction (AMI; RR = 1.42), disseminated intravascular coagulation (DIC; RR = 1.91), and immune thrombocytopenia (ITP; RR = 1.44). No statistical signals were identified following vaccination with either the mRNA-1273 or Ad26 COV2.S vaccines.
“Another thing, after receiving the vaccine, half of deaths were from effects on their nerves and heart, among the causes of death. You understand, right? Alpha, gamma, beta, and doing all that dumb stuff by gathering incompetent scholars, completely ignoring science and medicine. …This cannot happen ever again. This is a country of science and technology. Ignoring science and medicine, eroding our healthcare, it's a mess! Dream to reality, we're seeing how much urgent care we've had. Everyone that received this vaccine and had their blood pressure rise is all because of this vaccine. Nearly 2,000 people, but the actual deaths, I believe, are several times that. Most have given up hope. Given up hope, I say! They just so happened to conduct an autopsy and submitted an opinion piece, but it's left untouched! What are they doing? There's no reason to hide these facts.”
“Did you calculate the breakthrough infections? Most people were breakthrough infections. It's not the unvaccinated that are infected. It's the vaccinated that infect each other.The Ministry of Health and Labor publicized data that clarifies all of this. I will speak on this later.”
This data is “raw” and does not reflect any Under Reporting Factor - which could be far higher than the most rational estimates of 40 for the US and may be as high as 70 (h/t momo):
One paper that examined this issue identified seven regions of the spike protein which fulfilled the structural criteria necessary for the formation of amyloids, and when tested, these regions were found to cause amyloids to form. In the same way that the abnormal fibrous clots gradually build up within the vaccinated until a fatal tipping point is reached, I believe the same may also be occurring with amyloid depositing in the tissue (hence Pfizer’s recent investment in cardiac amyloidosis).
Others have also noticed the prion-forming characteristics of the spike protein. One of the most definitive reviews of the subject (by authors including Stephanie Seneff and Peter McCullough) highlighted a variety of mechanisms to explain the prion-forming behavior of the spike protein and its ability to enter the central nervous system (e.g. via the spleen where the vaccine nanoparticles were known to accumulate). Interestingly, authors also noted that of the variants, Delta (which my colleagues suspect was engineered) had a higher score for prionogenesis than the original Wuhan strain, whereas Omicron had a substantially lower score.
One in every 500 children under five years who received the Pfizer mRNA Covid vaccine were hospitalised with a vaccine injury, and one in 200 had symptoms ongoing for weeks or months afterwards, a study has found.
The study published in JAMA included 7,806 children aged five or younger who were followed up of for an average of 91.4 days following their first Pfizer vaccination. It was a retrospective cohort study done as an authenticated online survey (response rate 41.1%) in spring 2022 which included parents or caregivers who registered children for SARS-CoV-2 vaccination in outpatient care facilities in Germany. It compared the adverse events to those of the same children with other vaccinations in order to control for over-reporting.
You may find some of the following claims initially hard to believe. But we can assure you that each and every one has been extracted from official Government approved documents. If you are willing to read on then you are about to stumble on the most comprehensive selection of evidence that proves Covid-19 vaccination is in effect causing mass depopulation, and your Government knew it would happen. We will reference each and every document for you to “fact check” the claims yourselves.
Though the study’s authors tried their best to minimize the link, they were unable to sidestep a “positive association” between “vaccine-related aluminum exposure” and “persistent asthma” in children aged 24-59 months. Overall, children in the study who received 3 milligrams (mg) or more of vaccine-related aluminum had a 36 percent higher risk than children who took other vaccines to develop persistent asthma.
Note that a true vaccine-free placebo was not used in the study so as to make aluminum appear less damaging than it actually is. Had the study authors compared vaccinated children to unvaccinated children, the health risks associated with aluminum exposure would have been even more striking.
Using CDC and sponsor-reported adverse event data, we find that booster mandates may cause a net expected harm: per COVID-19 hospitalisation prevented in previously uninfected young adults, we anticipate 18 to 98 serious adverse events, including 1.7 to 3.0 booster-associated myocarditis cases in males, and 1,373 to 3,234 cases of grade ≥3 reactogenicity which interferes with daily activities. Given the high prevalence of post-infection immunity, this risk-benefit profile is even less favourable.
University booster mandates are unethical because: 1) no formal risk-benefit assessment exists for this age group; 2) vaccine mandates may result in a net expected harm to individual young people; 3) mandates are not proportionate: expected harms are not outweighed by public health benefits given the modest and transient effectiveness of vaccines against transmission; 4) US mandates violate the reciprocity principle because rare serious vaccine-related harms will not be reliably compensated due to gaps in current vaccine injury schemes; and 5) mandates create wider social harms. We consider counter-arguments such as a desire for socialisation and safety and show that such arguments lack scientific and/or ethical support.
We estimate that 22,000 - 30,000 previously uninfected adults aged 18-29 must be boosted with an mRNA vaccine to prevent one Covid 19 hospitalisation. Using CDC and sponsor-reported adverse event data, we find that booster mandates may cause a net expected harm: per Covid-19 hospitalisation prevented in previously uninfected young adults, we anticipate 18 to 98 serious adverse events, including 1.7 to 3.0 booster-associated myocarditis cases in males, and 1,373 to 3,234 cases of grade ≥3 reactogenicity which interferes with daily activities. Given the high prevalence of post infection immunity, this risk-benefit profile is even less favourable. University booster mandates are unethical because:
No formal risk-benefit assessment exists for this age group;
Vaccine mandates may result in a net expected harm to young people;
Mandates are not proportionate: expected harms are not outweighed by public health benefits given the modest and transient effectiveness of vaccines against transmission;
US mandates violate the reciprocity principle because rare serious vaccine-related harms will not be reliably compensated due to gaps in current vaccine injury schemes; and
Mandates create wider social harms. We consider counter-arguments such as a desire for socialisation and safety and show that such arguments lack scientific and/or ethical support.
Finally, we discuss the relevance of our analysis for current 2-dose Covid-19 vaccine mandates in North America.
The current research suggests the COVID shots altered the innate immune system, which is likely to alter the adaptive immune system.
…vaccinated individuals will have a reduced IFN-alpha/beta response and poorer immune clearance.
…Seneff said that the reduced symptoms in the vaccinated are likely because of this reduced pathway, since the initial symptoms of COVID-19 are caused by actions of the interferon action. This is why many vaccinated individuals are getting infected with rebound symptoms. “[The vaccinated] don’t get the symptoms…don’t feel as sick, but actually, you’re spreading the disease like crazy because you’re not fighting it off.” This also means that the virus will stick around in vaccinated individuals for longer, and if the disease is not cleared after a long period of time, it can cause severe disease down the line.
…recent studies have shown that innate immune function has been altered in those injected with the COVID shots. A preprint study found receptors that activate T cell action, including TLR7/8 (toll like receptors 7 and 8), are reduced in vaccinated individuals. Further, a Chinese study of people who have been vaccinated with the spike protein-inducing COVID-19 shots found that gene activity for what proteins and pathways are turned on and off have changed across most immune cells. The study found T cell activity was reduced as well as an increased inflammatory response in the immediate weeks following vaccination, which, in the long-term, puts people at risk for cancer.
“These data suggested that after vaccination, at least by day 28, other than generation of neutralizing antibodies, people’s immune systems, including those of lymphocytes (T cells, B cells, natural killer cells) and monocytes (innate immune cells), were perhaps in a more vulnerable state,” the authors wrote.
These findings overlap with pathologist Dr. Ryan Cole’s observations at his medical laboratory, Cole Diagnostics. Cole told Jan Jekielek on American Thought Leaders that after vaccinations started rolling out in the older population, he noticed the reappearance of Molluscum contagiosum, a parapoxvirus that most people get in childhood and is kept in check by the immune system from the teenage years onward. Though the uptick is unusual, as Cole saw more cases he grew concerned that the vaccines may be driving a form of “immune dysregulation,” meaning a possible breakdown to established immune controls. Since these viruses are normally kept in check by T cells, which also keep cancers in check, a loss of immune memory against viruses could be a sign of loss of control in cancers…
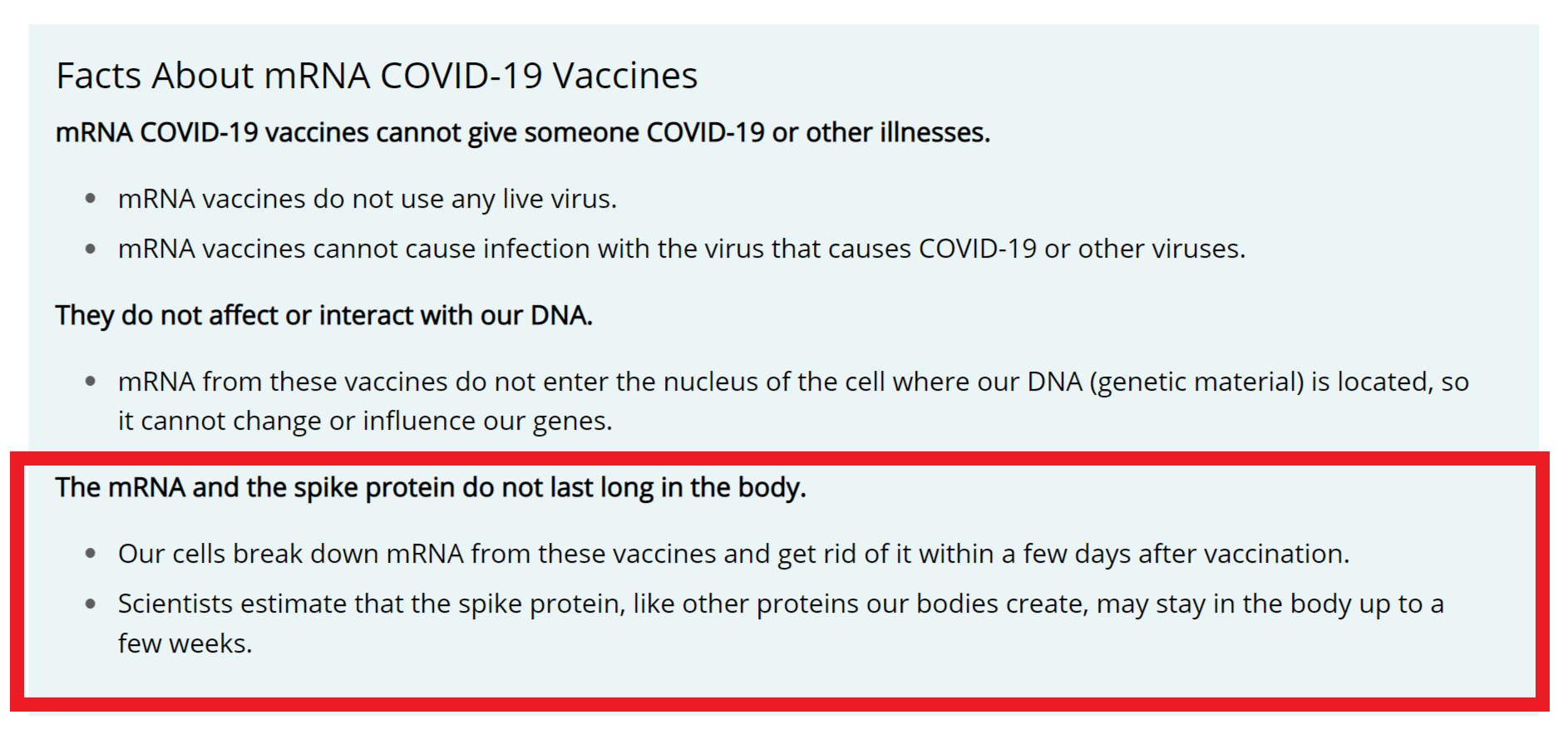
The text in the red box quietly disappeared. I.e., CDC admits it was all wrong. I.e., the mRNA and S spikes stay in the “vaccinated” for much longer than “few weeks”.
This study focuses on cardiovascular effects, particularly myocarditis and pericarditis events, after BNT162b2 mRNA COVID-19 vaccine injection in Thai adolescents. This prospective cohort study enrolled students from two schools aged 13–18 years who received the second dose of the BNT162b2 mRNA COVID-19 vaccine.Data including demographics, symptoms, vital signs, ECG, echocardiography and cardiac enzymes were collected at baseline, Day 3, Day 7, and Day 14 (optional) using case record forms. We enrolled 314 participants; of these, 13 participants were lost to follow up, leaving 301 participants for analysis. The most common cardiovascular effects were tachycardia (7.64%), shortness of breath (6.64%), palpitation (4.32%), chest pain (4.32%), and hypertension (3.99%). Seven participants (2.33%) exhibited at least one elevated cardiac biomarker or positive lab assessments. Cardiovascular effects were found in 29.24% of patients, ranging from tachycardia, palpitation, and myopericarditis. Myopericarditis was confirmed in one patient after vaccination. Two patients had suspected pericarditis and four patients had suspected subclinical myocarditis. Conclusion: Cardiovascular effects in adolescents after BNT162b2 mRNA COVID-19 vaccination included tachycardia, palpitation, and myocarditis.
The homologous recombination DNA repair pathway is one of the mechanisms that the body uses to stop your cells turning cancerous in response to environmental stress.
One of the most important components of this pathway is Tumor Protein P53 (p53), the “guardian of the genome”. It protects our cells from cellular damage. Under cellular stress, p53 jumps into action, regulating gene expression to control DNA repair, cell division and cell death. It is the most commonly mutated gene in cancer.
In October 2021, two revered scientists, called Jiang and Mei, had a paper published, after peer review, in the medical journal MDPI, showing that the SARS-Cov-2 spike protein obliterated the DNA repair mechanism in lymphocytes.
The viral spike protein was so toxic to this pathway that it knocked 90% of it out. If the whole spike protein got into the nucleus (in the ovaries), and enough of it was produced and hung around long enough before the body was able to get rid of it all, it would cause cancer. Fortunately, in the case of natural infection, this is unlikely to occur.
"Jakob Fuglsang, a cyclist ont the Tour de France : "Since my second dose of vaccine, I'm stuck". Breathing problems: (anonymous competitor) "Worst Tour of my career. I did my second dose before the Critérium du Dauphiné and since then, you can tell there has been some change." Lots of competitors "complain on the whole that they are not able any longer to push their breathing capacity to its paroxysm when the race crosses a certain threshold of intensity". According to Jakob Fuglsang: "Since my second dose I can't push my limits. (...) It's so frustrating because everything seemed perfect before the vaccine."
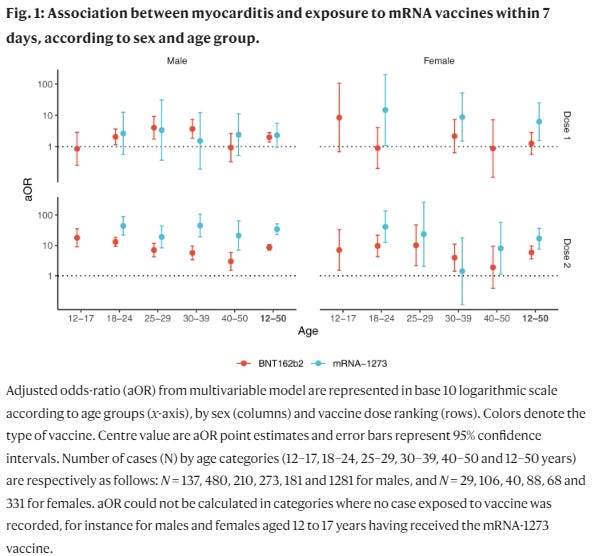
The risk of myocarditis was substantially increased within the first week post vaccination in both males and females (Fig. 1 and Table S2). Odds-ratios associated with the second dose of the mRNA-1273 vaccine were consistently the highest, with values up to 44 (95% CI, 22–88) and 41 (95% CI, 12–140), respectively in males and females aged 18 to 24 years but remaining high in older age groups. Odds-ratios for the second dose of the BNT162b2 vaccine tended to decrease with age, from 18 (95% CI, 9–35) and 7.1 (95% CI, 1.5–33), respectively in males and females aged 12 to 17 years, down to 3.0 (95% CI, 1.5–5.9) and 1.9 (95% CI, 0.39–9.3), respectively in males and females aged 40 to 51 years.
An increased risk of pericarditis was also found in the first week after the second dose of either of the mRNA vaccines among both males and females (Fig. 2 and Table S3). Odds-ratios for the second dose of the BNT162b2 vaccine showed a downward trend across age groups with values up to 6.8 (95% CI, 2.3–20) and 10 (95% CI, 2.5–41), respectively in males and females aged 12 to 17 years. The second dose of the mRNA-1273 vaccine was associated with pericarditis among males and among females only within age 30 to 39 years (odds-ratio 20 [95% CI, 3.5–110]) and age 40 to 50 years (odds-ratio 13 [95% CI, 3.5–49]).
Here, we present a comprehensive histopathological analysis of endomyocardial biopsies (EMB) from 15 patients with reduced ejection fraction (LVEF = 30 (14-39)%) and the clinical suspicion of myocarditis following vaccination with Comirnaty® (Pfizer-BioNTech) (n = 11), Vaxzevria® (AstraZenica) (n = 2) and Janssen® (Johnson & Johnson) (n = 2). Immunohistochemical EMB analyses reveal myocardial inflammation in 14 of 15 patients, with the histopathological diagnosis of active myocarditis according the Dallas criteria (n = 2), severe giant cell myocarditis (n = 2) and inflammatory cardiomyopathy (n = 10). Importantly, infectious causes have been excluded in all patients. The SARS-CoV-2 spike protein has been detected sparsely on cardiomyocytes of nine patients, and differential analysis of inflammatory markers such as CD4+ and CD8+ T cells suggests that the inflammatory response triggered by the vaccine may be of autoimmunological origin. Although a definitive causal relationship between COVID-19 vaccination and the occurrence of myocardial inflammation cannot be demonstrated in this study, data suggest a temporal connection. The expression of SARS-CoV-2 spike protein within the heart and the dominance of CD4+ lymphocytic infiltrates indicate an autoimmunological response to the vaccination.
“Analysis of Thromboembolic and Thrombocytopenic Events After the AZD1222, BNT162b2, and MRNA-1273 COVID-19 Vaccines in 3 Nordic Countries” (JAMA Network, 2022.06.14): “There was an observed increased rate of coagulation disorders following all 3 vaccines (AZD1222: RR, 2.01 [95% CI, 1.75-2.31]; BNT162b2: RR, 1.12 [95% CI, 1.07-1.19]; and mRNA-1273: RR, 1.26 [95% CI, 1.07-1.47]). There was also an observed increased rate of cerebrovascular disease following all 3 vaccines (AZD1222: RR, 1.32 [95% CI, 1.16-1.52]; BNT162b2: RR, 1.09 [95% CI, 1.05-1.13]; and mRNA-1273: RR, 1.21 [95% CI, 1.09-1.35]). For individual diseases within the main outcomes, 2 notably high rates were observed: 12.04 (95% CI, 5.37-26.99) for cerebral venous thrombosis and 4.29 (95% CI, 2.96-6.20) for thrombocytopenia, corresponding to 1.6 (95% CI, 0.6-2.6) and 4.9 (95% CI, 2.9-6.9) excess events per 100 000 doses, respectively, following AZD1222 vaccination.”
The decrease in immunity can be caused by several factors such as N1-methylpseudouridine, the spike protein, lipid nanoparticles, antibody-dependent enhancement, and the original antigenic stimulus. These clinical alterations may explain the association reported between COVID-19 vaccination and shingles. As a safety measure, further booster vaccinations should be discontinued. In addition, the date of vaccination should be recorded in the medical record of patients. Several practical measures to prevent a decrease in immunity have been reported. These include limiting the use of non-steroidal anti-inflammatory drugs, including acetaminophen to maintain deep body temperature, appropriate use of antibiotics, smoking cessation, stress control, and limiting the use of lipid emulsions, including propofol, which may cause perioperative immunosuppression. In conclusion, COVID-19 vaccination is a major risk factor for infections in critically ill patients.
This study provided in vivo evidence that inadvertent intravenous injection of COVID-19 mRNA vaccines may induce myopericarditis. Brief withdrawal of syringe plunger to exclude blood aspiration may be one possible way to reduce such risk.
“Remember when they said you were just as likely to get Myocarditis from Covid?“ (The Naked Emperor, 2022.06.02): “A study published last month in the Journal of Clinical Medicine on MDPI took a look at the incidence of myocarditis and pericarditis in post COVID-19 unvaccinated patients. COVID-19 did not increase the risk of myocarditis and pericarditis when compared with those who did not get Covid. These results tie in with a previous study in Nature, which I wrote about in April. This found a greater than 25% Increase in Cardiovascular events in under 40s during Vaccine rollout but NOT during Covid waves.“
“Unprecedented Number of Women Experience Rare Gynaecological Event“ (The Daily Expose, 2022.05.13): “Over more than 100 years, fewer than 40 cases of decidual cast shedding — during which the uterus’ thick mucous lining is shed, intact — have been reported. But over a 7.5 month period in 2021, 292 women experienced it, raising questions about whether Covid-19 vaccines could be to blame.“
“CG enrichment in covid vaccine mRNA“ (El Gato Malo, 2022.05.11): “Is this mRNA vaccine-cancer link proven beyond doubt? no. Is it suggestive enough to warrant A LOT of serious work? yes, i think so. Not having done this pre-release is a massive, monstrous lapse. The safety work here seems slipshod, incomplete, and short-term. None of these are things you look for in a product about to go into a billion people.“
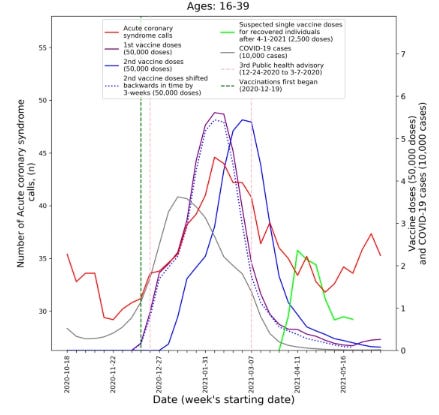
Weekly counts of acute coronary syndrome calls (five-week centered moving-average), COVID-19 cases (three-week centered moving-average), and vaccination doses (three-week centered moving-average) for those between 16 and 39 during: A) the study period (January 1st, 2019, to June 20th, 2021) and B) the third COVID-19 wave and vaccination distribution period (October 18th, 2020, to June 20th, 2021). COVID-19 Coronavirus disease 2019.
“Autopsy Histopathologic Cardiac Findings in Two Adolescents Following the Second COVID-19 Vaccine Dose“ (Archives of Pathology & Laboratory Medicine, 2022.02.14): “Results.– The microscopic examination revealed features resembling a catecholamine-induced injury, not typical myocarditis pathology. Conclusions.– The myocardial injury seen in these post-vaccine hearts is different from typical myocarditis and has an appearance most closely resembling a catecholamine-mediated stress (toxic) cardiomyopathy. Understanding that these instances are different from typical myocarditis and that cytokine storm has a known feedback loop with catecholamines may help guide screening and therapy.“
“A Moratorium on mRNA 'Vaccines' is Needed“ (Dr. Byram Bridle, 2022.04.21): In May 2021 I realized two things: 1. There was a lack of transparency about data supporting COVID-19 inoculations. 2. Incorrect messaging was being relayed to the public. On March 1, 2022 an English version of the biodistribution study was released. It contains much more information than the Japanese version I had looked at. Also, this accurate English language translation has revealed inappropriate biases in the conclusions drawn by the study director. Repeated administration of lipid nanoparticles, especially over a limited period of time, is known to be toxic. This included an interview with the Chief Executive Officer of Moderna and others in the biotechnology industry. Here are quotes from the hyperlinked article:
“In nature, mRNA molecules function like recipe books, directing cellular machinery to make specific proteins. Moderna believes it can play that system to its advantage by using synthetic mRNA to compel cells to produce whichever proteins it chooses. In effect, the mRNA would turn cells into tiny drug factories. It’s highly risky. Big pharma companies had tried similar work and abandoned it because it’s exceedingly hard to get RNA into cells without triggering nasty side effects.”; “Delivery — actually getting RNA into cells — has long bedeviled the whole field. On their own, RNA molecules have a hard time reaching their targets. They work better if they’re wrapped up in a delivery mechanism, such as nanoparticles made of lipids. But those nanoparticles can lead to dangerous side effects, especially if a patient has to take repeated doses over months or years. Novartis abandoned the related realm of RNA interference over concerns about toxicity, as did Merck and Roche”.
A key question is to what degree are these toxicities additive? Unless lipid nanoparticles are definitively proven safe in humans, their repeated administration to people should be avoided.
• mRNA vaccines promote sustained synthesis of the SARS-CoV-2 spike protein.
• The spike protein is neurotoxic, and it impairs DNA repair mechanisms.
• Suppression of type I interferon responses results in impaired innate immunity.
• The mRNA vaccines potentially cause increased risk to infectious diseases and cancer.
• Codon optimization results in G-rich mRNA that has unpredictable complex effects.
“SARS-CoV-2 Vaccination and Myocarditis in a Nordic Cohort Study of 23 Million Residents“ (JAMA Cardiology, 2022.04.20): “Findings: In a cohort study of 23.1 million residents across 4 Nordic countries, risk of myocarditis after the first and second doses of SARS-CoV-2 mRNA vaccines was highest in young males aged 16 to 24 years after the second dose. For young males receiving 2 doses of the same vaccine, data were compatible with between 4 and 7 excess events in 28 days per 100 000 vaccinees after second-dose BNT162b2, and between 9 and 28 per 100 000 vaccinees after second-dose mRNA-1273.“
“Persistent Cardiac MRI Findings in a Cohort of Adolescents with post COVID-19 mRNA vaccine myopericarditis“ (The Journal of Pediatrics, 2022.03.25): “Repeat cardiac magnetic resonance (CMR) imaging was performed within 3-6 months to guide next clinical decision-making steps; timing was modified in some individuals based on scanner accessibility and safety precautions during the COVID-19 pandemic. Although symptoms were transient and most patients appeared to respond to treatment (solely with NSAIDS), we demonstrated persistence of abnormal findings on CMR at follow up in most patients, albeit with improvement in extent of LGE.“
Here, we highlight a case of a 64-year-old woman who presents with rapidly declining memory loss, behavior changes, headaches, and gait disturbance approximately one week following administration of the second dose of the novel Pfizer-BioNTech messenger ribonucleic acid (mRNA) COVID-19 vaccine.
mRNA contained in the Pfizer-BioNTech COVID-19 vaccine has the potential to bind to specific proteins and cause pathologic misfolding.
• Various portions of the COVID-19 mRNA Pfizer-BioNTech vaccine to have a high affinity for cytoplasmic proteins such as TAR DNA binding proteins (TDP-43) and Fused in Sarcoma (FUS) .
• Spike protein, which is translated by the mRNA, can increase intracellular zinc, which has been shown to cause the conversion of TDP-43 into its pathological prion.
• Kuo et.al demonstrated how TDP-43 binds to mRNA transcripts with long UG-repeats.
• Pfizer-BioNTech’s COVID-19 vaccine contains many of these specific sequences.
• Tetz and Tetz identified a prion-like domain found in the receptor-binding domain of the S1 region of the SARS-CoV-2 spike protein.
“Sars-Cov-2 Kills T-Cells, Just Like HIV” (Igor Chudov, 2022.03.14): “Sars-Cov-2 destroys immune T cells just like HIV does, Sars-Cov-2 has a transplanted gp120 HIV insert, and it is that specific gp120 insert that allows HIV to enter lymphocytes via the same LFA-1 receptor!“
“Pathologist on Ryan Cole on the mystery blood clots” (RUMBLE, Steve Kirsch, 2022.03.14): “caused by S spike, in his honest opinion” (and here’s another Rumble video discussing the weird clots - https://rumble.com/vtr470-worldwide-exclusive-embalmers-find-veins-and-arteries-filled-with-never-bef.html)
“VACCINE RECKONING: More than 66% of “fully vaccinated” Israelis are now suffering adverse reactions” (Natural News, 2022.03.04)": “Israel’s Ministry of Health published data from a recent survey showing that more than 66 percent of the people in Israel who got fully injected, then “boosted,” suffered some kind of reaction to the shots that has made living normal life much more difficult. Some 2,049 citizens were asked three to four weeks after getting a third “dose” of a Fauci Flu shot how they feel now. Most of them revealed that they feel terrible, and roughly half of them say that carrying out normal, everyday activities is now exceptionally difficult.“
“Myocarditis Following COVID-19 BNT162b2 Vaccination Among Adolescents in Hong Kong” (JAMA Pediatrics, 2022.02.25): “43 adolescents had myocarditis-related hospitalization following receipt of BNT162b2 vaccination, and 84% of the hospitalizations (36 of 43) occurred after the second dose. The incidence rate was 3.12 (95% CI, 1.25-6.42) and 22.15 (95% CI, 15.51-30.67) per 100 000 persons for the first and second dose, respectively.
Among the 343 700 adolescents in Hong Kong, no COVID-19-related death has been reported, and the only one admitted to the pediatric intensive care unit due to COVID-19 was an imported case,5 indicating that the risk of death or complications from COVID-19 is extremely low among adolescents in Hong Kong. Vaccination policy for adolescents should consider the trade-off between risks and benefits. “
The myocardial injury seen in these postvaccine hearts is different from typical myocarditis and has an appearance most closely resembling a catecholamine-mediated stress (toxic) cardiomyopathy. Understanding that these instances are different from typical myocarditis and that cytokine storm has a known feedback loop with catecholamines may help guide screening and therapy.
“What happens to those billions of NanoParticles you've become host to?” (Marc Girardot, 2022.02.11): “The number of nanoparticles (NP) injected in a dose of these anti-COVID vaccines is utterly flabbergasting: up to 50 billion viral vectors for AstraZeneca, 40 billion LNPs for Moderna, and likely 10 billion for Pfizer. It’s not very clear how many intact messenger RNA are in each LNP , but even if we agree to only 1, and that each one produces 1000 spike protein, we are talking your body having to deal with a minimum 30 trillion pathogenic spike proteins in a few months time… The worse case scenario is certainly a direct intravenous injection because a concentrated dose naturally leads downstream to a concentrated transfection in a large area that it was never supposed to reach. That would lead to an extremely brutal reaction, a cytokine storm of epic proportion, major thrombosis, and most likely rapid death given the number of LNPs injected. An indeed as early as March 2021, the Danish authorities have been recommending to use the aspiration technique to avoid such occurrences.“
“Embalmers Find Veins & Arteries Filled with Never Before Seen Rubbery Clots“ (Steve Kirsch, 2022.01.28): “Funeral Director and embalmer Richard Hirschman reveals, for the first time ever, arteries and veins filled with unnatural blood clot combinations with strange fibrous materials that are completely filling the vascular system. He has gone from seeing 50% of his embalmed cases with these types of blockages rise to almost 80%. It only started happening after the vaccines were rolled out.“
“Whistleblowers share DOD medical data that blows vaccine safety debate wide open” (Hotowitz, 2022.01.26): On Monday, during Sen. Ron Johnson’s five-hour hearing on a “COVID-19: Second Opinion,” Ohio attorney Thomas Renz, who has been representing clients suing the vaccine mandates, presented DOD medical billing data from the Defense Medical Epidemiology Database (DMED) that paints a shockingly disturbing picture of the health of our service members in 2021:
300% increase in DMED codes registered for miscarriages in the military in the first 10 months of 2021, compared to 5-year average (4,182 from 1499)
300% increase in cancer diagnoses (from a five-year average of 38,700 per year to 114,645 in the first 11 months of 2021)
1,000% increase in diagnosis codes for neurological issues, which increased from a baseline average of 82,000 to 863,000
myocardial infarction –269% increase
Bell’s palsy – 291% increase
congenital malformations (for children of military personnel) – 156% increase
female infertility – 471% increase
pulmonary embolisms – 467% increase
“Booster Shots causing more cases of Lymphadenopathy” (The Naked Emperor, 2022.01.24): “…boosters cause a 13 fold increase in cases of lymphadenopathy[compared to double-jabbed]! Almost 1 in 20 people having the Pfizer vaccine report these swellings. The side effect should be moved from the ‘Uncommon’ column to the ‘Common’ (>1/100 to <1/10) one.“
“Norway Raises Concern Over Vaccine Jabs for the Elderly“ (Bloomberg, 2022.01.16) : ”Norway expressed increasing concern about the safety of the Pfizer Inc. vaccine on elderly people with serious underlying health conditions after raising an estimate of the number who died after receiving inoculations to 29.”
“SARS-COV-2 Vaccines and Neurodegenerative Disease” (The Epoch Times, 2022.01.11): “Our paper showed that there are several mechanisms by which these vaccines could lead to severe disease, including autoimmune disease, neurodegenerative diseases, vascular disorders (hemorrhaging and blood clots) and possibly reproductive issues.“
“Cerebral venous thrombosis after vaccination against COVID-19 in the UK: a multicentre cohort study“ (The Lancet, 2021.09.25): “Between April 1 and May 20, 2021, we received data on 99 patients from collaborators in 43 hospitals across the UK. Four patients were excluded because they did not have definitive evidence of cerebral venous thrombosis on imaging. Of the remaining 95 patients, 70 had VITT and 25 did not. The median age of the VITT group (47 years, IQR 32–55) was lower than in the non-VITT group (57 years; 41–62; p=0·0045). Patients with VITT-associated cerebral venous thrombosis had more intracranial veins thrombosed (median three, IQR 2–4) than non-VITT patients (two, 2–3; p=0·041) and more frequently had extracranial thrombosis (31 [44%] of 70 patients) compared with non-VITT patients (one [4%] of 25 patients; p=0·0003). The primary outcome of death or dependency occurred more frequently in patients with VITT-associated cerebral venous thrombosis (33 [47%] of 70 patients) compared with the non-VITT control group (four [16%] of 25 patients; p=0·0061).“
Enter your suggestions in the comments section below.
































https://rumble.com/vqx3kb-the-pfizer-inoculations-do-more-harm-than-good.html
https://www.vacsafety.org
https://odysee.com/@TimTruth:b/fauci-pushes-force-vax:b
https://odysee.com/@TimTruth:b/vaers-sudden-deaths:d
https://odysee.com/@TimTruth:b/Yeadon-fuellmich-premeditated-mass-murder:4