Adolescents aged 13–18 were studied in a prospective cohort manner just after the second injection of the Pfizer vaccine and 7/301 (23,256/million or about 2.3%) developed myocarditis using a clinical definition based on blood tests, ECG, and cardiac imaging. Data from multiple sources suggest the condition can be subclinical in about half, meaning neither the patient nor the parents bring it to clinical attention.What’s more, 7/202 boys had overt or subclinical myocarditis (3.5%).
Then I have stumbled over this video, quoted in “Evidence of harm” (Steve Kirsch, 2022.09.21):
This study raises an important issue for the repeated periodic “boosting” with mRNA jabs:
Evaluating the true incidence is of major importance, as this information is required for informed decision making for patients,physicians, and public health authorities given the apparent need for repetitive (possibly yearly) booster vaccinations for billions of humans worldwide due to diminishing protection months after the last COVID-19 vaccination.
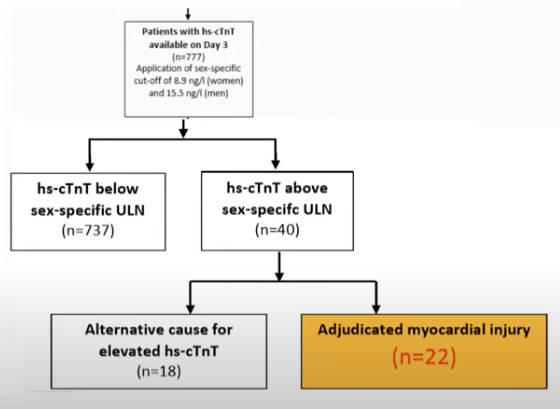
The study subjects were monitored via a troponin test Day 3 after a booster jab. If found elevated, also tested on Day 4, and had a complete medical evaluation on Day 30. If there were any reasons to suspect any cause other than the booster, myocarditis was attributed to that cause instead. So, the most conservative estimate of the myocarditis incidence in this study has been 22 out of 777 study subjects (>2.8%, or 1 in 35), another 18 cases attributed to other possible causes.
Conclusion: Using active surveillance mRNA-1273 vaccine-associated myocardial injury -likely indicating myocarditis- was found to bemuch more common than previously thought. It occurred in one out of 35 persons, was mild, and more frequent in women versus men.
Being mild or not mild is not the point here. The point is, you get the cumulative heart muscle injury with every subsequent booster jab and, as we know, the heart muscle damage is irreversible (e.g., this [Google-trusted] source says that “after a heart attack, the adult human heart has a low regenerative capacity. The body replaces cardiomyocytes at a rate of 1% per year at age 25 and 0.45% per year at age 75.”).
The Swiss study presentation also includes this slide, showing the cumulative proportion of troponin levels measures in the study subjects (grey - unvaccinated controls, black - “boosted”)
Red lines/pink shading added by me (read below):
A few words of explanation are on order so that this slide can be understood and interpreted correctly. First, the hs-cTnT concentration on the horizontal axis seems to display wrong units:ng/L instead of ng/mL. I assume it must be ng/mL, else the numbers do not make sense as being 1000 times too small to mean anything. Next, the dashed vertical lines are different for females and males: about 8ng/mL for women and 17 ng/mL for males. This seems to be the sex-specific cut-off troponin levels for the subclinical myocarditis. This is corroborated by the corresponding numbers for the acute myocardial events to be taken as 16 ng/mL for women and 34ng/mL for men in “Sex-Specific Cut-Offs for High-Sensitivity Cardiac Troponin: Is Less More?” (Hindawi, 2019):
Apparently, the Swiss study took 50% of the acute myocarditis cut-off levels to be the cut-off levels for the subclinical myocarditis.
Next, there is always some troponin level present, and the 3ng/mL was measured in about 30% of women, and 10% of men in the study, boosted or otherwise. From there up, the grey and black lines diverge, the black line indicating elevated troponin levels the in boosted for 70% of women and for 90% of men, be it however small, compared with unboosted.
We can see that some controls (women and men) also exhibited elevated levels of troponin above the cut-off levels (the grey and black lines above the horizontal red lines added by me).
The controls had been enrolled prior to Covid-19. Therefore, the troponin measurements for matching controls have been taken from before Covid-19, so no Covid-19 jabs in the controls.
Also, this study only tracked the first 30 days post booster, who knows what happens after the curtain is dropped... So, 1 in 35 is only the tip of the iceberg, the number for a year may be much greater as we know the spike may be produced in the jabbed for about 5 months, give or take (“What If S Spike-Targeting Jabs Never Worked, Like At All?”, 2022.06.02).
Watch the video to get the complete scoop on this study. Even better, if anyone is a member of the European Society of Cardiology, could you please download the video and the presentation slides from the ESC web site here and forward them to me? Unfortunately, these documents have restricted access and haven’t been published anywhere else (wonder why). I don’t want to get Prof. Mueller into any further trouble by requesting these from him directly and then reposting them here.
So, 1 in 35 (or 1 in 40) gets at least mild myocarditis following a single Pfizer booster, most likely more with the Moderna and Pfizer bivalent marvels of $cience. That is about 1 student per every high school class here in North America, most conservatively. Or, as they say, exceedingly rarely.
A longtime British radio host died of a suspected heart attack on Monday, while presenting his daily segment on the air, his radio station announced.
Tim Gough, 55, died early Monday morning while his show "Tim Gough at Breakfast" aired live, GenX Radio said in a news release. Gough was presenting the show from his home in Suffolk, the county in east England where he was born.
Under how much physical exertion should have he been, presenting the talk show from home? Of course, we can rule out any boosters as a probable cause?
This is awesome information, thanks for sharing! It's obvious that any type of vaccine mandate for kids absolutely will send some of them to the hospital -- for a disease that they aren't at risk of in the first place. This is the type of information we have to give to school boards or whoever else is going to ultimately make these decisions.
In either case the answer is SAFE PREVENTION ~ as discovered, described and heralded by our martyred scientists and physicians espousing safe, inexpensive generic meds and supplements ~ now including nasal and oral rinses. And healthy diets, exercise, etc. Homicidal damaging uncaring Big Pharma go home.








This is awesome information, thanks for sharing! It's obvious that any type of vaccine mandate for kids absolutely will send some of them to the hospital -- for a disease that they aren't at risk of in the first place. This is the type of information we have to give to school boards or whoever else is going to ultimately make these decisions.
In either case the answer is SAFE PREVENTION ~ as discovered, described and heralded by our martyred scientists and physicians espousing safe, inexpensive generic meds and supplements ~ now including nasal and oral rinses. And healthy diets, exercise, etc. Homicidal damaging uncaring Big Pharma go home.